One evening in early March, after completing the first day of her ambulatory medicine clerkship rotation, Celestine Warren ’21, received some unsettling news.
“I got a call saying that there had been a COVID-19 exposure at Dartmouth and that our clinical training was being suspended for two weeks,” recalls Warren, a fourth-year medical student at Dartmouth’s Geisel School of Medicine. With the subsequent cancelling of all non-essential patient care, the clerkships, which provide in-person clinical training to third- and- fourth-year medical students, would end up being discontinued. “It was a tumultuous period. We were all feeling scared and uncertain and trying to figure what to do. As we quarantined, we continued with clerkship-related activities at home as best we could.”
Warren reached out to one of her preceptors, Alison Romegialli, MD, an assistant professor of medicine at Geisel. “I asked if I could call in on my rotation days so I could join the virtual patient visits she was setting up and she agreed—that was a turning point,” she says. “We worked out a system wherein we’d have a conversation via conference call and then after the patient would hang up, we’d be able to debrief, and she could teach me. I’d do things like print out a cognitive impairment screening on my home computer, score it by myself, then we’d go through it together after to see how I’d done.
“I was thankful to be able to get an educational experience out of it, both primarily in ambulatory medicine which was my goal, but also in seeing how a health system can reorganize and adapt and what kinds of care can still be evaluated and delivered on the phone,” says Warren, who was one of a small number of medical students at Geisel to complete a clerkship rotation remotely during the early days of the pandemic.
Forced Innovation
Dartmouth-Hitchcock Health (D-HH)—which includes a network of hospitals and clinics throughout New Hampshire and Vermont and serves nearly two million people—was no stranger to delivering virtual care prior to the pandemic.
Established in 2012, Dartmouth-Hitchcock Connected Care and Center for Telehealth had grown to include seven service lines. The six acute care, on-demand services are TeleEmergency, TeleNeurology, TeleICU, TelePsychiatry, TelePharmacy, and TeleICN—where specialists are available around the clock to assist local care teams with orders, diagnosis, patient management, and transfer recommendations. The seventh service, Outpatient Virtual Visits, refers to scheduled outpatient appointments directly with providers, most commonly to patients’ homes. Since its inception, the center had provided tens of thousands of telehealth encounters and had been involved with the review of approximately two million medication orders.

As part of the only academic medical center in the state and one of only three in Northern New England, the center’s mission has been to help deliver outstanding care to the region independent of patient location and with a major focus on rural care since many regional hospitals that D-HH supports are smaller critical care hospitals in remote locations that lack good access to specialists.
“A lot of people don’t know about it, but in recent years we’ve become probably the most mature telehealth center in New England and one of the more mature centers east of the Mississippi as the numbers go, particularly in terms of acute, on-demand inpatient and emergency department care,” says emergency medicine physician Kevin Curtis, MD, MS, medical director for Connected Care and an associate professor of medicine at Geisel.
Standing in stark contrast were outpatient visits, where the vast majority of medical care is conducted. “Prior to the pandemic, we were only doing about eight a day total, and that was across 30 specialties in 14 locations. All of a sudden, the demand for virtual outpatient visits exploded—at our peak, I think we maxed out at about 2,600 a day,” says Curtis. “Since then, we’ve settled back down to about 600 a day but with a total of over 150,000.”
A number of factors facilitated this exponential increase. Because of the state of emergency brought on by the pandemic, many of the restrictions that had slowed the growth of outpatient virtual care in the past such as those involving insurance reimbursement, licensing, and patient privacy were relaxed. That left many providers scrambling to quickly find virtual solutions for their practices—from SBR Vidyo (D-HH’s legacy platform), Doximity, and WebEx to the telephone.
“In the face of need, people innovate, and they do it really impressively,” says Peter Solberg, MD, an HIV medicine physician and chief health information officer at D-HH who serves as an associate professor of medicine at Geisel. “Everything was happening at ‘warp speed’ compared to how these things normally get done. Our technical teams, both on the IT side and the telehealth side, have been stretched thin but they’ve done a lot of great work in supporting as many of these activities as possible.”
At the same time, the teams have continued to work on a longer-term, scalable solution involving D-HH’s Epic electronic health record and Zoom. “The new Epic/Zoom video visits went live in mid-September, and I think it’s safe to say we are all pretty enthused about the new opportunities it presents,” says Solberg. “For example, the new platform allows us to bring multiple users into an ambulatory visit, including a trainee who might be somewhere removed from both the patient and the provider.”
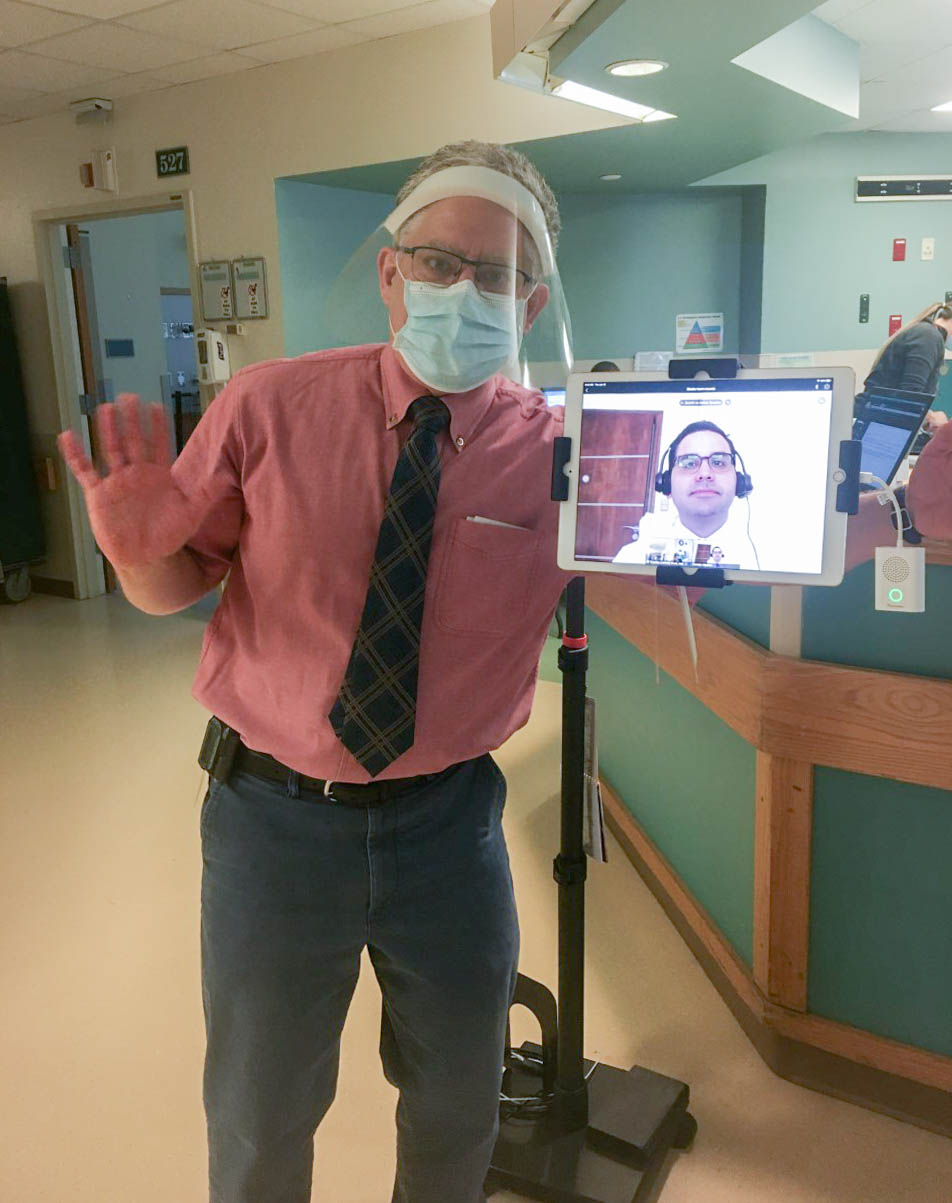
On the inpatient side, the teams worked to deliver care in new ways in response to the pandemic. This included deploying 18 telehealth carts around the region to hospitals that don’t normally have tele-ICU capabilities (and four in D-H’s non-ICU cohort units) in case of a surge in COVID-19 cases. They also used tablets across the medical center to preserve supplies of PPE and limit the exposure of clinicians, allowing them to provide care from outside patients’ rooms from within the hospital, as well as from beyond the hospital walls.
Incorporating Learners
With the dramatic increase of telehealth activity seen across D-HH those working in medical education at Geisel saw an unprecedented opportunity to include medical students in a patient care process that would inevitably be part of their future.
“We suspended all educational activities for our students for about three months when COVID-19 hit,” recalls hospitalist John Dick III MED ’03, interim senior associate dean of medical education and an assistant professor of medicine at Geisel. “We were following AAMC guidelines on that, and so that really then pushed us to say, ‘Well, what other ways can we get our students involved in patient care?’”
Dick and his colleagues put out a call to faculty across the institution, saying, “’We’ve got our clinical students who right now we’re not permitting to be in the hospital or the clinics: what sort of virtual learning activities do you have?’ But many people were just starting to get comfortable with using virtual technology and were still working through some of the technical difficulties that came up.”
“I think that those attending physicians who were able to answer the call were incredibly innovative in the middle of all of this to be able to include learners as they did,” says Curtis.

One of those physicians was Timothy Lukovits, MD, a stroke neurologist at D-HH and an associate professor of neurology at Geisel. “We were receptive to doing it because we’d gained some experience with it, including introducing the technology to our residents,” says Lukovits, “and we saw it as a way to help enhance their education, not just from a technology standpoint but from what it’s like to provide care in a regional center that works with a lot of disparate areas.”
In addition to being one of the earliest adopters of telemedicine in the region, Lukovits had established a tele-neurology elective for residents and was starting to do inpatient rounds and virtual shared visits with associate providers to expand stroke care coverage—using an iPad and D-HH’s TeleNeurology platform. During the pandemic, he also helped to pilot a more user-friendly form of Webex’s video conferencing software for D-HH providers.
“Over the years, we’ve learned how to examine patients in the emergency department or inpatient setting, and things like how to position the equipment and optimize lighting, and this helped us to work out some of the kinks we ran into early on and make it a better learning experience for students.”
Lukovits worked with Geisel medical students Oliva Sacks MED ’20 and Damian Almiron Bonnin ’21, helping them to fulfil their neurology rotations virtually. “I found it quite a positive experience,” says Bonnin, who had been visiting his family in Paraguay and couldn’t return to the U.S. during the pandemic. “We used the electronic medical record with an iPad Pro with special videoconferencing microphones and speakers so that I could participate fully in the patient visits.
“However, what really made the experience successful was our team of educators,” says Bonnin. “They were clearly passionate about teaching the next generation of physicians on the field, and I was lucky enough to have the chance to learn from them. Residents and attendings were insightful, helpful, and always willing to try new things to improve the virtual learning environment. Dr. Lukovits, for example, worked closely with me to research and implement a new piece of technology for teleconferencing that significantly improved the quality of the virtual clinical interactions.”
Virtual Primary Care
Another D-HH physician answering the call was Leah Matthew, MD, an assistant professor of community and family medicine and of medical education who worked with Geisel medical students Patrick Tolosky ’21 and Frank Zhang ’21 to develop a modified preceptor-student model which allowed them to participate in their family medicine clerkships remotely.
“It just felt important to get them re-engaged—it was very clear early on that students wanted to be doing more than just virtual learning,” says Matthew, who directs the family medicine clerkships at Geisel. “Some of the early challenges that we had to work through included the fact that many of us in our practice were learning to use telehealth for the first time, and there hadn’t been a script for how to have students involved with it or how to give them feedback.”
Also, because of some systems limitations, they weren’t able to use three-way video, says Matthew, so the students did the virtual patient visits by phone. “But I was excited about how it really wasn’t that much extra work to include them, and the students did a great job of both being involved initially as ‘guinea pigs’ and of providing critical input to the process,” she says.

“In the beginning, I was a little bit nervous about using just the phone and perhaps missing some of the details that you pick up in face-to-face meetings with patients,” says Tolosky. “But I feel like I got the hang of it pretty quickly and realized that it was quite similar to our normal office interactions.”
The process included huddling in the morning to do a brief preview of the patients that day. “Then I would call the patients about a half hour before their scheduled time to ask them about any symptoms they were experiencing, the medications they were taking, and other things like exercise and diet,” he says. “Afterward, I would gather my thoughts and call Dr. Matthew to debrief her on the patient and discuss next steps. Then, she’d do the virtual visit with the patient and link me in so I could listen and chime in if needed.
“It was great to be able to interact with patients during that difficult time. Telemedicine allowed us to address their acute health concerns, or refill a prescription, or just listen for a few extra minutes about their day or a personal struggle—I found that to be grounding amidst all of the turmoil and challenges of COVID-19,” says Tolosky. “I think telemedicine is here to stay. And getting exposure to it as medical students can only help us in terms of being able to meet the needs of our different patient populations in the future.”
Looking Ahead
Dick and many of his colleagues in medical education at Geisel share that same view. “I think there is a commitment amongst the faculty and a recognition that telemedicine is a vitally important area to educate our students on,” he says. “But we’re still very much at the starting point curricular-wise on this, in terms of figuring out how to move forward and what it might look like.”
Under consideration, is to incorporate it into Geisel’s On Doctoring program, a two-year course (in years 1 and 2) that typically uses standardized (hired and trained) patients in the simulation center at Dartmouth-Hitchcock Medical Center to introduce medical students to essential clinical skills through longitudinal clinical and small group learning experiences.
“I think introducing telemedicine to students early on—when they’re first focusing on things like patient interviewing, physical diagnosis, clinical reasoning, and communication skills as they begin to develop the doctor-patient relationship—would allow us to establish it as an important option in patient care, particularly in rural settings like ours,” says Roshini Pinto-Powell, MD, a professor of medicine and of medical education at Geisel, and a long-time advocate for including telemedicine in clinical training. Pinto-Powell is co-director of On Doctoring with Adam Weinstein, MD.
“To me, education should follow clinical care, meaning that we shouldn’t just do something because it’s innovative in the education space,” she says. “We should do it because it’s of value and we’re trying to create doctors who will have the skills to practice in many different settings and circumstances in the future. I think that future definitely includes telemedicine.”