
Alumni Album:
John Kattwinkel, M.D., '66: The reluctant doctor
by Laura Stephenson Carter
Doctors in the University of Virginia's neonatology division use space-age technology-like microprocessor-controlled ventilators- to save the lives of tiny babies. They're babies who almost certainly would have died if they'd been born in the 19th century, when division director John Kattwinkel's ancestors were practicing medicine in rural Vermont. Kattwinkel comes from a long line of doctors, one of whom, family lore has it, delivered the first baby at Burlington's Fletcher Allen Hospital in the late 1800s.
"My mother went by horse and buggy with her grandfather to make house calls," Kattwinkel recalls. She once watched as a patient was held down on a kitchen table so her grandfather could do a tonsillectomy. And Kattwinkel's father, an internist, was chief of medicine at Newton-Wellesley Hospital in Massachusetts.
But Kattwinkel wasn't interested in entering the family business. "I had so many doctors in my background that I wasn't going to be one," he confides. Instead, he studied mechanical engineering at Rensselaer Polytechnic Institute (RPI). The call of medicine was irresistible, however. He switched his major to biology and began to think about going to medical school. "My father was so proud that I was going to join the crew and become a doctor," Kattwinkel recalls.
After graduating from RPI, he enrolled in DMS's then two-year program. "It was wonderful when I got into Dartmouth," he says. "It was like a gift from above . . . that's where my roots are." After graduating from DMS, he completed his M.D. at Harvard in 1968. He was doing his residency at Duke when he decided to specialize in neonatology. Sadly, the impetus was the death of his infant daughter. She had a congenital heart defect-hypoplastic left heart syndrome, in which the left side of the heart is underdeveloped-and died when she was just three days old. "It was an emotional time for me," Kattwinkel says. "Why should she be a beautiful, healthy-looking girl and be dead two days later?"
Now the once-fatal syndrome can be treated with a series of operations or a heart transplant. Doctors and parents examine the complex medical and surgical options together before choosing a course of action. In the 1960s, however, even if such treatment options had been available, parents would have been excluded from the decisionmaking. Doctors wanted to "protect" parents from having to make painful choices. "I knew it was wrong," Kattwinkel says. "I'm sure that had a lot to do with my decision to go into neonatal care."
After further training in clinical research at the National Institutes of Health (NIH) and a neonatology fellowship at Case Western Reserve Medical Center under respiratory neonatologist Marshall Klaus, M.D., known for his theory of maternal-infant bonding, Kattwinkel was named director of the Division of Neonatology at the University of Virginia in 1974. He has been there ever since.
At Case Western, Kattwinkel started researching apnea-an unexpected cessation of breathing-and respiratory distress syndrome (RDS). He even invented a device to treat RDS by gently forcing air into a premature baby's immature lungs. He has also investigated artificial surfactant-another way to treat RDS. The syndrome is caused by a lack of surfactant, a foamy fluid that reduces surface tension in the lungs' air sacs and thus allows them to inflate.
Since he has been at UVA, Kattwinkel has organized several multicenter randomized clinical trials to determine the most effective strategies for administering surfactant. It turns out that it is more effective if given to preemies earlier than had been the practice.
Kattwinkel has also been looking at how surfactant is administered as well as when. Typically, surfactant has been delivered through a tube inserted in a baby's windpipe. But recently, he says, "we've been looking at giving surfactant during the birth process." It appears to be more effective if it is put in the baby's mouth as its head crests in the mother's birth canal. The new technique has been tested on 24 babies, and Kattwinkel is looking for funding to conduct more trials.
In the late 1970s, Kattwinkel received an NIH grant to develop an educational initiative called the Perinatal Continuing Education Program (PCEP). Its goal is to teach medical personnel how to stabilize very sick or premature babies before they're transferred from local hospitals to tertiary medical centers. The program has been implemented in hundreds of hospitals in over 40 states; more than 100,000 providers in this country and in U.S. military hospitals overseas have participated. PCEP has also been adapted for use in Poland, Mexico, Bosnia, China, and Canada. "We use his outreach education model here, too," says Dartmouth neonatologist George Little, M.D.
But Kattwinkel's best-known contribution to neonatal care-one that even garnered him an appearance on the Today show-was alerting the public to the fact that certain sleeping positions increase the risk of sudden infant death syndrome (SIDS). He chaired the American Academy of Pediatrics (AAP) Task Force on Infant Sleep Position, which evaluated studies from Europe, Australia, and New Zealand suggesting that babies who sleep on their stomachs are more apt to succumb to SIDS. Once known as "crib death," SIDS is the sudden, unexpected death of a baby who's under one year old. About 6,000 infant deaths a year were attributed to SIDS in the early 1990s. No one understood what caused it. But doctors had been advising parents to have babies sleep on their stomachs so if they happened to throw up, they'd be less likely to aspirate their vomit.
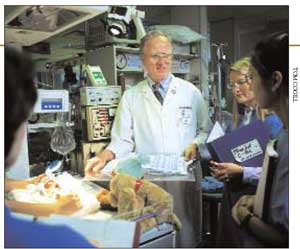 Photo by Tom Cogill A neonatologist at the University of Virginia, DMS alumnus John Kattwinkel is slated to be featured in July on the Discovery Channel and in U.S. News & World Report. |
"I was not involved with SIDS before," Kattwinkel says. "The Academy was looking for someone who didn't have an agenda. So they chose me." His threemember task force included John Brooks, who at the time was at the University of Rochester and in 1994 became chair of pediatrics at Dartmouth. To be sure, there were a lot of strong opinions on the subject. Some people thought SIDS was related to apnea. Others believed the culprit was toxic fumes in mattresses. Still others were sure SIDS was due to an infection.
But, says Kattwinkel, "the evidence was overwhelming that babies who slept on their stomachs had a two- to five-times increased chance of dying of SIDS." Ironically, about a year before the task force was convened, Kattwinkel had visited hospitals in China and seen babies there sleeping on their backs. "I told [the doctors] it was dangerous," Kattwinkel confesses. The Chinese doctors promptly turned the babies onto their stomachs. "But when I came back a little while later, the babies were all back on their backs," Kattwinkel chuckles. "Asians have always put babies on their backs." It seems the Chinese had the right idea, though U.S. doctors didn't know it at the time.
So, says Kattwinkel, "the NIH very wisely set up an annual survey to see how babies were being placed for sleep. We all chewed our fingernails for the first year." The survey confirmed what researchers in other countries already knew: that babies who sleep on their stomachs are at higher risk for SIDS. In 1992, the AAP recommended that babies be put to sleep on their backs. And in 1994, Kattwinkel helped launch the national "Back to Sleep" campaign.
The number of SIDS cases is now half what it used to be. Each year, says Kattwinkel, "there are 2,500 fewer babies dying." That means more than 10,000 children are alive today who might have been victims of SIDS had there not been a change.
"Now we think SIDS is related to rebreathing and carbon dioxide," he explains. "The groundbreaking research came out of Dartmouth." DMS pediatrician James Filiano, M.D., and Hannah Kinney, M.D., a neuropathologist at Children's Hospital in Boston, found that an abnormality in the brain stem appears to inhibit the babies' ability to regulate their breathing.
Kattwinkel has also addressed a few other issues related to SIDS. Some SIDS deaths have been associated with suffocation in stuffed toys, comforters, pillows, or loose bedding. So the U.S. Consumer Product Safety Commission and the AAP have revised their recommendations on safe bedding practices for infants. In addition, the task force has determined that babies whose mothers smoked during their pregnancy are at higher risk for SIDS. Kattwinkel suspects that there may be a connection between maternal smoking and the brain-stem abnormality. The risk of SIDS is higher in childcare centers, he adds, so there's a new "Back to Sleep" campaign aimed at secondary caregivers.
Kattwinkel has become involved in the area of neonatal ethics, too. In the late 1980s and early 1990s, he was a founding member (and later the cochair) of the Neonatal Resuscitation Program Steering Committee of the AAP and the American Hospital Association (AHA). And he's currently the editor of the awardwinning AAP/AHA Textbook of Neonatal Resuscitation.
"It's not the prematurity that is associated with bad outcomes. It's all the complications that occur," he explains. "The problem is, when they're born, you don't know what the complications are going to be. It's very difficult not to resuscitate a baby [who has problems]. Our position is that it's more ethical to intervene in the beginning and then stop" rather than to never intervene.
Kattwinkel is now helping to develop new AAP guidelines to de- fine how small is too small. Under the current guidelines, resuscitation is not recommended for a preemie who is born after less than 23 weeks' gestation or who weighs less than 400 grams. Babies born after 25 weeks or weighing at least 1,000 grams have better outcomes. "But now we're agonizing over the gray zone," says Kattwinkel- babies who are born at 23 to 25 weeks' gestation or who weigh 400 to 700 grams.
Kattwinkel was recently selected as a recipient of the Discovery Health Channel's first-ever Medical Honors. He and 12 other clinicians will be celebrated for their achievements in a broadcast scheduled to air in July. In addition, U.S. News & World Report will feature the Discovery Channel honorees in its annual "America's Best Hospitals" issue, also due out in July.
"He's really a true triple-threat person," says Dartmouth's Little, referring to the fact that medical academicians strive to excel in clinical care, research, and education. "He's known as an excellent clinician, an excellent laboratory and clinical researcher, and an excellent educator-with his perinatal continuing education program."
Even though he once resisted becoming a doctor, John Kattwinkel would surely have made his physician-ancestors proud.
If you would like to offer any feedback about this article, we would welcome getting your comments at DartMed@Dartmouth.edu.