
An Audacious Effort
By Drew Remignanti, M.D., M.P.H.
Smallpox was eradicated worldwide in the 1970s, and the hope is that within a few years polio, too, will have been wiped from the face of the earth. A Dartmouth grduate who spent two months in Pakistan helping with that audacious, but probably attainable, effort tells his story by way of photos and the e-mails he sent home.
Remignanti, a 1975 graduate of Dartmouth College, practices emergency medicine in Manchester, N.H. He earned his M.D. from Rutgers and an M.P.H. from Medical College of Wisconsin. Remignanti spent the months of May and June 2000 in Pakistan, taking part in that country's polio eradication initiative through a program of the U.S. Centers for Disease Control and Prevention and the World Health Organization; his participation was also supported by Rotary International, a major funder of the global polio eradication effort. The main part of this feature consists of the actual emails that Remignanti wrote to friends and family during his time in Pakistan; they have been edited only slightly for publication. He welcomes hearing from anyone interested in polio eradication at the e-mail address listed on the messages here.
From: "Drew Remignanti, MD" <drew1r@pol.net>
Sent: May 23, 2000 12:28 PM
Subject: Polio Eradication 101
Greetings from Quetta, Balochistan, Pakistan. I've been here almost a month, but haven't had a chance to write everyone yet. I heard today that it was 50*C (around 120*F) south of here, while it was merely in the 90s here. Quetta gets only two to four inches of rain a year and even less currently due to the drought. Consequently, the surrounding mountains and everything else are khaki-colored (khaki actually being a local word in Pashto meaning "dust"), with a few splashes of green where there's irrigation. I'm embarrassingly but gratefully housed in a very luxurious hotel paid for by my CDC/WHO (Centers for Disease Control/World Health Organization) per diem allowance.
At a quick glance, polio would seem a very easy disease to eradicate: its symptoms are easily recognizable; you can test for the virus in stool instead of blood; the virus can't be transmitted by animals or insects; there's an excellent oral vaccine that anyone can administer (hence pictures of President Clinton and others giving "polio drops"); and just three doses establish immunity in American kids. But on the flip side: for every one infected person who exhibits paralysis, there can be 100 to 200 people who are infected but have no symptoms; kids growing up in tropical, developing nations need many more doses to become immune (malnutrition weakens their immune response, and contaminated drinking water gives them other intestinal viruses that interfere with their response to the polio vaccine); both the vaccine and any stool waiting to be tested must be kept refrigerated (which can be tough in 120* climates with poor access to electricity and transportation); and the virus is highly contagious through simple contact.
The first country to eradicate polio was actually Cuba, in 1962 (of course, if I wanted to eradicate an infectious disease I'd probably want to be a dictator on an island, too). After that achievement, the Pan American Health Organization felt challenged to match it. They started seriously pursuing polio eradication in 1985 and had eradicated polio throughout the Americas by 1991. WHO made the same decision in 1988, but Africa and Asia made serious efforts starting only in the early 1990s—so the virus is now concentrated on those continents.
To get around the difficulties I described above, WHO has developed a clever scheme to accomplish worldwide polio eradication. The first step is repetitive dosing with vaccine through national immunization days (NIDs), on which millions of kids are dosed on the same day or two, twice in one month. The second step is what they call acute flaccid paralysis (AFP) surveillance. Rather than training people to specifically diagnose polio, they are asking people to report anything that looks like it might be polio (there are a dozen or more conditions that can look similar in the initial stages); then WHO staff revisit and stool-test those kids. This achieves two things: it shows where the virus is, so they know where to concentrate further vaccination efforts, and it develops a system sensitive enough to not miss any poliovirus, which is critical for accurately assessing whether the virus is completely gone. The experience in the Americas and elsewhere has shown that for a population of kids under age 15, there is at least one case of AFP that's not polio per every 100,000 kids. So if a country is not finding that many cases, its AFP surveillance program is deficient.
Of the eight of us here with the Stop Transmission of Polio (STOP) team, four of us are helping to improve the NIDs, while the other four, including me, are working on the AFP surveillance efforts. I guess this has been a long-winded answer to the question, "So, what are you going to be doing, Drew?"
Regards, Drew
From: "Drew Remignanti, MD" <drew1r@pol.net>
Sent: May 28, 2000 1:51 AM
Subject: Polio Found
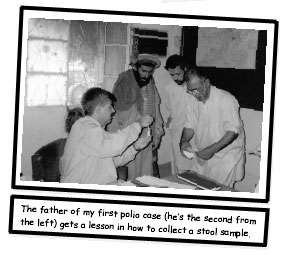
Saw my first polio case yesterday—a three-year-old boy with a twoweek history of a paralyzed left leg. He was brought in by his father and his eight-year-old sister. They're Afghan refugees in a village here in Quetta. Neither child had received any routine immunizations, but they had gotten three doses of polio drops on the NIDs, which would have been enough in the developed world to cause immunity. Both kids were undernourished and small for their ages, but either the girl became immune while the boy didn't or—more likely —she was among the 99% of those infected with polio in whom it doesn't cause paralysis (luck of the draw either way).
It was hard to rely on the father's history, since he was illiterate and unaware of what day of the week or even month it was. We wanted to interview the mother to get a more accurate history of the illness before we determined for sure that it was polio, because it might be too late to find virus in the stool (assuming the father even returns with the stool samples; he had to go back to work, so we gave him the stool collection kit and a cooler to take with him). But the father refused to consider letting us meet the mother because she "keeps purdah," meaning she has no contact with any man other than her husband (that's another of the barriers to polio eradication in Pakistan!).
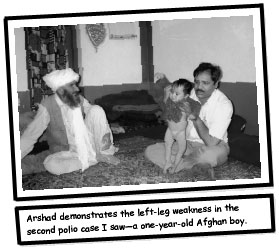
Then I saw my second case today. It was a follow-up visit on another Afghan boy, one year old, who'd originally come in with left-leg paralysis. His stool test had shown definite polio type 1 virus (there are actually three types, so you could theoretically get polio three separate times, although the vaccine protects against all three).
Again, he'd had no routine vaccinations and only three supplemental doses on the NIDs. We went out to his house to do the mandatory 60-day follow-up exam to check for residual weakness, which he clearly had. It was a good opportunity to see how people live. His village area was a mix of brick/concrete and mud-walled/tent dwellings. His was concrete, with electricity and an overhead fan, so his family was relatively well off compared to others nearby. (The first case had been brought directly to our office building and can really only be called AFP at this point, even though the experienced people said it was classic polio. Ideally, that boy will be exam- ined again in 60 days, too, and if he has residual weakness will be presumed to be a polio case even if his stool samples are not returned properly.)
There are about a dozen or so other conditions (other enteroviruses, Guillain-Barre syndrome, and other neurological diseases) that can look like polio in the beginning, but they differ in not leaving a child with residual weakness two months later. The way the system is set up now, children who die or are otherwise lost to 60-day follow- up—by moving to some unknown part of Afghanistan, for ex- ample—are classified as polio cases on the strength of the initial evaluation. This may overestimate the incidence of polio somewhat, but the decision was made to err on the side of overdiagnosis at this stage. Right now, however, Pakistan is in the midst of moving from a clinical diagnosis scheme—based on observation of weakness at the 60-day visit—to a virological classification system. Under this sort of system, if two good stool specimens show no virus, the case is discarded as non-polio; and if virus is found, then it's clearly polio. The tougher cases (where the stools are inadequate in some way or other problems arise) are reviewed by an expert committee—including a virologist, a pediatrician, a neurologist, and an epidemiologist—that also has the option of choosing a third diagnostic category called "polio compatible."
Getting polio was obviously terrible luck for these two kids, but my having seen these cases has helped to make this effort feel more worthwhile. The Pakistan numbers look good, though. They had 3,000 cases of polio in 1994, when they first started the NIDs and AFP surveillance, then 1,000 in 1997 and only 500 in 1999; the rate of cases in 2000 has so far been slower yet. Clearly, the WHO deadline of polio eradication by 2000 has been missed, but perhaps in another year or two, if the enthusiasm and effort can be kept up, it'll be over.
Regards, Drew
From: "Drew Remignanti, MD" <drew1r@pol.net>
Sent: June 6, 2000 1:53 AM
Subject: Delhi Belly
I'm in the recovery phase of what travelers in India call "Delhi belly" — your basic gastrointestinal upset. I'm still feeling washed out, but I put my GI tract through a successful stress-test last night. I hooked up with Julia and Bonnie (two of the other STOP team docs) and Jean Welsh (a permanent, full-time WHO employee in Islamabad—an impressive commitment, since women are totally marginalized here), and we went to the United Nations club for dinner. Like the American club, it is an oasis of Western culture, offering a temporary escape; there's a pool, alcohol is served, and Western-type foods are on the menu. I feasted on garlic bread and spaghetti with meat sauce, followed by an ice cream sundae.
Alcohol is, of course, officially banned in Pakistan because of the Muslim influence. It's available only in clubs or higher-class hotels, which have signs in the rooms that say, "Alcohol available by special order for non-Muslim guests." Previous STOP teams told me that private consumption in homes is not rare, however. My office address in Quetta is, in fact, Brewery Road; I haven't seen the actual brewery yet but have been told that "they can't legally sell in Pakistan" (sounds like a great business plan!). I don't know if there is a legal intoxicant here, but apparently in Karachi and parts of Balochistan, heroin production and use is heavy.
I don't know if there's a Pakistani phrase equivalent to Delhi belly; in fact, Pakistan and India don't seem to share much, except a mu tual animosity and distrust, at least at a public level. The historical roots of this conflict are fascinating and were completely new to me. I've learned that due to violent Hindu-Muslim relations, Pakistan was carved out of India in 1947, at the time India achieved independence from Britain. This was done to accommodate the Muslim community, which wanted a separate homeland. Since there were no natural geographic boundaries along which the division could be made, relatively arbitrary ones were drawn. The huge Punjab province was split and, with areas to the west, became West Pakistan, while what is now Bangladesh split off to become East Pakistan; though separated by 1,000 miles, the two regions formed the united Muslim country of Pakistan, "Land of the Pure." Since 1971, though, Bangladesh has been an independent country.
This geographical split was also the origin of the Kashmir issue. Technically known as AJK (Azzad Jammu and Kashmir), this region was a conglomeration of separate "khanates," or kingdoms, which didn't want to go either way. It was decided to, in a sense, set them aside and let them vote on their choice at a future date. This vote has never taken place (this is India's fault, apparently, since an early vote would likely have gone Pakistan's way)—hence the chronic conflict in the region over ownership.
At the time of partition, what I'm told was the largest migration ever took place, with Muslims and Hindus fleeing in fear in opposite directions to relocate on the "right" side of the boundary. It's said that in the ensuing chaos and violence, between 200,000 and 1,000,000 people were killed. Knowing this history makes the roots of the current distrust more understandable.
I haven't been near the Indian border, but I've heard and read that even though there are still Hindus in Pakistan and Muslims in India, some families split during the partition and have never visited each other since. Interestingly, this affects the epidemiology of polio, in that Pakistani poliovirus is more likely to be similar to strains found in Iran or Afghanistan than to those in India. Enough blather—apparently I'm feeling better. Hope all is well with everyone at home.
Regards, Drew
From: "Drew Remignanti, MD" <drew1r@pol.net>
Sent: June 8, 2000 10:45 PM
Subject: Stalking the Wild Poliovirus
"Wild poliovirus" is actually a term that is used to distinguish the disease-causing virus from the live-vaccine virus, both of which can be found when testing patients' stool specimens; it felt like we were stalking it today. I finally got the chance to escape the urban setting. Dr. Sarfraz (the provincial AFP surveillance officer and thus my local counterpart), a driver, and I drove two hours south out of Quetta to the Kalat district, taking Lak Pass through the mountains into the plains. We could see the broader Bolan Pass in the distance, which, along with the more renowned Khyber Pass, was considered the most likely route that an invading Russian Army would take after passing through Afghanistan to attack India—something England spent most of the 19th century worrying about. As it turned out, it was England that occupied parts of Afghanistan twice in that century, while Russia made its invasion attempt only recently. Each was thrashed soundly in its turn. (In the first English retreat from Kabul, it's said that of 16,000 soldiers and civilians who started off marching back to India, winter and Afghani tribesmen killed all but one.)
The mountains and scrubby vegetation make Balochistan look very similar to the U.S. Southwest. Outside the city, many of the dwellings are a smooth mud-and-dung construction that looks identical to our Southwest's adobe-type buildings. From the main road, you can see many temporary tent compounds belonging to nomads who migrate to higher altitudes in the summer, seeking better pasturage for their sheep, goats, donkeys, and camels. (It's a nice change seeing these animals in a more natural setting. On the streets of Quetta, they have to compete with the cars; the sheep and goats always seem to make the least movement necessary to avoid impact, apparently having a false sense of security due to their numbers. The donkeys are constantly clip-clopping along the streets, pulling carts that are called "tongas," with a frantic look of worry on their faces. In contrast, the occasional camel is always the quintessence of cool, loping along and covering twice the distance with half the effort.)
The nomad tents thinned out as we descended to the plains, and the heat and humidity rose. We were in a modern vehicle with seatbelts, four-wheel drive, and air-conditioning. The road, surprisingly, went from very good to perfect on a long stretch recently built by the Iranian government (apparently to make their trucking to and from Karachi more convenient). In Kalat, we visited the district health office and hospital, where I was able to give my little canned AFP surveillance talk to a receptive group of a dozen medical officers and related staff. This stimulated them to tell us of a child whom they had just sent home because they were uncertain what to do with him. He was a four-year-old boy who'd had paralysis of his left arm beginning after a minor fall three days ago, but his arm showed no obvious sign of injury. They knew only his village's name (Tok), not his or his parents' names.
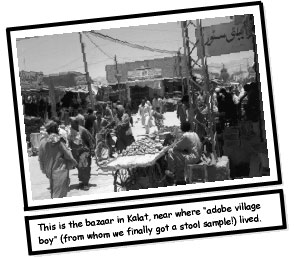
As it turned out, we were heading that way to go to the Khuzdar district anyway. So we drove several miles down the suggested dirt road, through the scrubby brush toward distant hills (not into the sunset yet, though it felt like a Western movie set). My companions started asking everyone we came across if they knew of a boy with a lame left arm. Unbelievably, we ended up in this "adobe" village (up close you can see the grain fibers in the final dung coating on the buildings), surrounded by a peach and apple orchard, in a room with 10 to 15 men and a smattering of children—one of whom was our "case investigation subject."
Then the typical problem arose, because the men were not able to answer questions like "Was the child ill with a fever when the prob- lem began?" To their credit, rather than feign knowledge they didn't have, the men ran back and forth between us and the boy's mother, relaying our questions and then her responses; but the simple solution of having the mother sit with us, even just to talk about her child's illness, was inconceivable.
It turned out to be a true AFP case (whether it's polio or not remains to be seen). Although an injury preceding AFP is generally a reason to exclude the case, we agreed with the hospital docs that there was a complete lack of bruising, swelling, or tenderness in the limb. The child could hold a peach in his left hand, but had to transfer it to his right hand to raise it to his mouth! The peaches were just a little bigger than walnuts at this stage, but we ate a few to be polite because we had to stay for tea anyway. The wonders kept coming, as we found out that the building we were in actually had both electricity and a refrigerator. We were able to instruct the father in how to collect and refrigerate two stool specimens, which we plan to pick up on our way back to Quetta on June 11. The boy's apparent lack of a fever and the fact that the affected limb is an arm instead of a leg argue against polio, while the fact that the boy's shoulder muscles are weaker that his forearm argue for polio—so it's a coin-toss at this point.
But fortunately our timing was perfect, and with such good (collected early and kept cold) stool specimens, the lab should be able to find poliovirus if it's there. It may just turn out that a case which would otherwise have been ignored will be proven to be polio; and even if it's not polio, it will contribute to the needed non-polio AFP statistics. The amazing thing is that this is precisely one of the main things they trained us for at the CDC—to try to find and encourage the local medical staff to report anything even remotely resembling polio. What a great feeling!
After two more hours of driving south, we finally reached Khuzdar at sundown. I'm right now in a local hotel, where a room costs 200 rupees a night ($4.00)—with no extra charge for the large black ants in the bathroom; at least they appear to be driving off the small black ants. But despite the low price, there's a ceiling fan, air-conditioning, good lights (and, for the moment, electricity to run them), and a toilet as well as a shower. What more can one ask for?
Regards, Drew
From: "Drew Remignanti, MD" <drew1r@pol.net>
Sent: June 10, 2000 11:48 PM
Subject: Balochi Road Trip
The rest of my weekend road trip has gone successfully, though June 8th was clearly the high point.
When I awoke the morning of the 9th, I discovered that three armed guards had been posted outside our hotel all night long. Dr. Sarfraz explained that this had been the decision of the district commissioner (DC) and was for my protection against "thieves and dacoits." When I asked if theft was a big problem in the area, he said no, but that if anything had happened to us it would have looked bad for the DC so he figured it was a reasonable precaution to take.
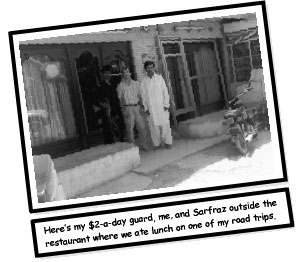
Then one of the guards—a Pakistani police officer who bore an impressive rifle, complete with a banana-shaped bullet clip—accompanied us all day in Khuzdar, for which I ultimately paid him 100 rupees ($2.00). He managed not to shoot anyone on my behalf and even ate lunch with us in a local diner-type place, sitting there with his rifle on his lap the whole time we were eating.
We then drove four more hours south until we reached the Lasbela district, on the coast. We were in and out of mountains with an endless variety of geologic forms, including a mini "redrocks" area with pink, red, purple, and black rocks. At Lasbela, the landscape flattens out into a sandy, Saudi Arabian-type look, with small dunes, cactuses, palms, camels, and banana groves.
The Arabian Sea is as warm as bathwater. The area is not likely to develop a tourist industry soon; where we stopped was "the largest ship-breaking area anywhere." They sail huge, outdated oil-tankers bow-first right onto the beach and haul them further up with tractors and huge chains. Then they proceed to strip the hulls down to skeletons to reuse their parts and metal. It's a much more functional, though not very aesthetic, use of waterfront property than we might choose. I'm sure there are probably nicer areas of beach, but this is what Sarfraz and Bakhtiar, our driver, seemed proud to show me after I asked to see the ocean.
We ended up in the town of Hab. Here, Sarfraz met up with a number of his medical school classmates and I gave another AFP surveillance presentation. I'd also given one earlier in the day in Khuzdar. After the Khuzdar presentation, I saw a sad case of a four-year-old girl with left-leg polio that she had contracted three years ago, despite receiving the full, routine three doses of oral polio vaccine (OPV). Part of the heartbreak was the fact that her father was the town's pediatrician, and he was wracked with sadness and guilt over her disability (she can walk and run, but with a significant limp). He said his colleagues give him a hard time, saying, "Look, he's the town's pediatrician and even his child has polio." He grilled me about new polio treatments like acupuncture and asked me to examine Bushra's leg to see if I thought surgery would help her, since I was the "senior doctor and expert." Needless to say, I felt a bit like a fraud. But at least I could tell clearly that even though her leg was atrophied and her Achilles tendon needed stretching to avoid further contracture, she did not need surgery yet. I promised her father that I would do an extensive search of the latest medical literature about acupuncture and other novel therapies for polio (although I'm relatively sure there are none).
Sarfraz and I both emphasized to him that there was nothing he could have done to avoid her illness and that some kids just don't develop immunity without the extra OPV doses that she would ultimately have gotten through the NIDs. We chose to use my role as "expert" to tell him (truthfully) that physical therapy and no restrictions on her activities would be the best treatment for her. I added that he would likely only bring stress-related illness on himself and his family if he didn't set aside his worry about why it had happened and what he could have done to prevent it. I don't know if he can, though. (Through all this, the mother, of course, sat mutely in the background with her head and face covered).
In Khuzdar, we had also gone on a search for a recently reported AFP case whose address was "village near airport road," but we weren't able to repeat our success of the 8th. In addition, we did a 60-day follow-up on an AFP case and luckily found a four-monthold boy, who had presented with paralysis of both legs, now vigorously kicking both legs. In the interim, his mother had taken him to a local surgeon, who had inexplicably put heavy plaster casts on both lower legs. I'm sure this didn't contribute to his recovery (the baby must have had one of the forms of non-polio AFP), but kicking his legs with those weights on them was doing a good job of building up his thighs.
Hab is the last town in Balochistan just before you reach the Sindh province. We skipped going the extra 15-minute drive to reach Karachi (a huge, urban sprawl, I'm told), because it's not our territory. We stayed the night in a real dive of a guesthouse for $10.
After the talk and the beach trip, plus many meetings in the towns of Uthal and Bela and much tea-drinking (a daily requirement in Pakistan), it was back north to Khuzdar on the 10th. It was triple-H weather—hot, humid, and hazy—with the only unique part being the haziness. Going through the mountains toward dusk, you could look right at the perfect disc of the sun through the thick haze. We stopped along the road where a well and pump were irrigating a field, to drink from the fresh, "safe" water. The field was sown with sunflowers and "oilseed" plants, along with cucumbers; we picked, washed off, and ate whole cucumbers as a snack.
Tonight we're staying in the same dive of a guesthouse again on our way back north, and tomorrow's plan is to revisit the earlier AFP cases, to try to find "airport road girl," to pick up the stool specimens from "adobe village boy," and then to head back "home" to Quetta. That's more than enough for now—I'll tell you a little more about the driving itself later.
Regards, Drew
From: "Drew Remignanti, MD" <drew1r@pol.net>
Sent: June 12, 2000 1:13 AM
Subject: Balochi Road Trip, Part II: Pakistani Realities
To start on a lighter note, I awoke on the morning of the 11th to find six armed guards outside our rooms—though "only two of them were for you," the rest being for some local prominent judge, according to Sarfraz. But presumably if the "dacoits" coming after me had overwhelmed my two guards, the others would have felt obliged to help out.
Now for the bad news: I felt like I was body-slammed back to earth on our return trip to Quetta. In Khuzdar, we learned that they had been making announcements in all the mosques within an eightkilometer radius, in an attempt to turn up the "airport road girl"— but still with no success. Getting people to obtain all the appropriate info on their initial contact with a patient is an uphill battle. Then we stopped in Tok to pick up the stool specimens from "adobe village boy," only to find that rather than the two refrigerated specimens we had requested, they had collected just one and had "left it in the shade" (it was probably 80-degree shade)! This was despite the fact that Sarfraz had gone through the explanation four times to a roomful of 15 adult men. I could have cried or screamed. I restrained myself, however, and confined myself to melodramatic pacing and brooding—raising my hands in the air and repeatedly muttering, "Such a simple idea," as if by osmosis or the power of repetition this guy who spoke no English would understand the importance of what we wanted.
The guy who was there when we returned was not the father, and he said that the parents were being uncooperative. Apparently they kept saying that it couldn't be polio, and they were convinced it was from the phantom injury; I hope they're right, but I doubt it — at least in terms of the injury. It may or may not be polio, but there's only one way to know. Sarfraz attributed our difficulty in conveying the seriousness of the situation to the general lack of education in Pakistan (the literacy rate is 50% for men, 25% for women, and under 10% for rural women), and he told stories of having received specimen containers filled with urine and collection kits with stool mixed in with water and ice. The fact that this simple process couldn't be pulled off under apparently ideal conditions, given local realities, left me feeling temporarily pessimistic about eradicating polio in Pakistan. The way we left things—after repeated explanations and demonstrations of the proper technique—was that the local district surveillance officer would persist in trying to get adequate stool specimens.
Based on my one afternoon of monitoring what are known as subnational immunization days (SNIDs), which are conducted on a doorto- door basis, as well as on the more extensive SNID experiences of others in my group, it's clear that many people here in Pakistan are making phenomenal efforts to eradicate polio. Just imagine if you were asked to knock on the door of every home in your own town and convince the parents to let you immunize all their children under age five for a disease that is now relatively uncommon. Now imagine doing it for more than 20 million children spread over an area larger than France, in 100-degree weather, for the grand sum of 80 rupees ($1.60) a day. And, furthermore, imagine having to deal with the refusal of people who believe it's a surreptitious form of birth control—a not uncommon belief here. I'm sorry, but I'm sure I'd drop out by day two. But it's expected that this will likely have to be done twice a year for the next two to three years—and that's just in Pakistan; similar efforts will be required in each of the remaining countries where polio is still endemic! We never had to do this in the U.S., by the way, because our kids responded readily to good routine immunization practices.
Here's an interesting polio factoid: In the U.S., there were 58,000 cases of paralytic polio in 1952. Ironically, the fact that we had a clean drinking-water supply worked against us to some degree. Kids were not exposed to poliovirus early in life, when they would have been more likely to come down with a simple, febrile form of the illness that would confer immunity to a more full-blown case. So when they were exposed to the virus later on, we had large epidemics every summer, with many paralytic cases.
I'll be off on another three-day road trip to two more districts, starting on the 15th. I'll let you know what that turns up.
Regards, Drew
From: "Drew Remignanti, MD" <drew1r@pol.net>
Sent: June 13, 2000 9:15 PM
Subject: Traffic laws?? We don't need no stinking traffic laws!!
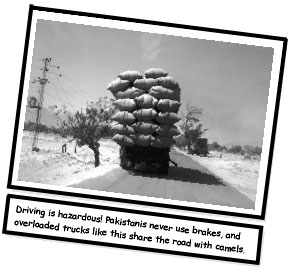
I'm convinced that if Pakistan ever produces an automobile, it will
come equipped with two extra horns and no brakes. Here, stepping
on the brakes is apparently seen as undermining the purpose of
motorized travel—that is, to maintain maximum velocity. There
are no posted speed limits in Pakistan; "speed limit" here is a concept
related only to a vehicle's intrinsic mechanical capabilities.
I also can't detect any enforced traffic laws—merely traffic suggestions, the primary one being that when outnumbered or outweighed, stay to the left. Even this suggestion is suspended if the vehemence of one's horn-blowing can convince obstructing objects to look to their own survival first. The preferred place to drive is directly down the center of the road, unless, of course, the pavement is in better condition in the other guy's lane, in which case it's firstcome, first-served.
Actually, I see Pakistani drivers as more opportunistic than aggressive. They rarely miss an opportunity to pass slower traffic, even if said opportunity happens to present itself on an uphill blind curve.
However, our driver, Bakhtiar, has earned my trust. I've come to look forward to driving as a form of entertainment; it's kind of like being in the chase scene of a grade-B movie, where they don't have the budget to actually smash up cars so they have to rely on scenes of near-impact for excitement. It's truly amazing how fast one can drive down a narrow, uneven side road filled with pedestrians and goats without leaving physical injury in one's wake. It would be an overstatement to say that Bakhtiar uses good judgment in his driving, but he's shown he can apply just the necessary amount of judgment. It's only on rare occasions that he manages to do something which, up until the very instant he pulls it off, I'm sure is impossible (these situations usually involve fitting our vehicle through an inadequate space at an alarming speed). Most of the time, his driving decisions are merely inadvisable.
Bakhtiar is a gruff but friendly guy, in his fifties, I'd guess, with a command of about a dozen English words—though I'd bet that he probably understands much more than he lets on. He likes to listen to loud Pakistani/Balochi mostly-melody-deficient music. When he needs to converse with Sarfraz, who sits in the back seat, Bakhtiar prefers to raise his voice to a decibel level sufficient to pierce through the music, thereby saving himself the effort of repeatedly adjusting the tape-player's volume.
I'm very disappointed that I can't understand a word that Bakhtiar says, because I would love to know how he expresses himself. He and I seem to have developed an indirect form of communication, however, in that when his horn-honking goes from its usual insistent but intermittent status to a continuous tone, I know it's time for me to look about us and attend to our predicament. Conversely, when my hand goes out to the dashboard (he can't detect my foot pressing firmly on the floorboards in the hope of finding a nonexistent brake pedal), he seems more likely to resort to his own rarely invoked brake pedal. I've tried not to abuse this motion for fear that it might lose its efficacy.
The passenger capacity of vehicles here is another fluid concept. It's not unusual to see a family of five on a single motorcycle (father driving, one child in front of him, and the mother on the back with a child on each knee—but nary a helmet in sight). Another variation is two men and a sheep on a motorcycle. And one day, outside a hospital, I saw a motorcycle bearing a threesome; the first man was driving and the third one, on the back, was holding up a unit of blood that was being actively transfused into the second man (one can only pray that they were leaving the hospital against medical advice). The passenger limit for trucks, vans, and buses is dictated only by the boldness of those willing to ride on top (which is also a popular spot for sheep or goats).
Amazingly, actual motor vehicle accidents seem rare, however. I've only seen firsthand the aftermath of one, and I read about another in the newspapers. Fortunately, in the one case I saw, a rollover, there were no human casualties and only a couple of mortally mangled sheep—though that was potentially a significant financial loss to somebody. My guess, though, is that the accident was not a lost opportunity but that it merely moved forward the moment of the beasts' metamorphosis into mutton! Mmmmmmmm, good. Uh-oh—it looks like I've run out of m's, so I'll have to go now. I'll write ore toorrow.
Regards, Drew
From: "Drew Remignanti, MD" <drew1r@pol.net>
Sent: June 18, 2000 11:16 PM
Subject: Inshallah
First, a stool-specimen update: Defying all odds, the local staff in Kalat succeeded in collecting appropriate stool samples from "adobe village boy" (by the way, Eric, one of my STOP colleagues, measured the temperature in the shade one day—it was 100.5*F!). In addition, the uneducated father of the first Afghan boy I saw, the one with AFP, returned with two good samples in the cooler we had given him (something that I had written off in my mind as extremely unlikely). In the next month or two, when the results from the lab tests and the follow-up exam are completed, I'll let you know if these cases turned out to be polio or not, inshallah.
That phrase—inshallah, or "God willing"—is a constant refrain here. I haven't been able to decide if it represents a true spiritual sense of detachment and acceptance of God's omnipotence and of our limitations or not. There have been many moments when I've felt it was more like a "manana attitude" tricked out in fancy-dress clothes.
One day, when I was making arrangements to ship home a carpet I'd bought, the merchant concluded with the statement, "It will arrive at your home in one to two weeks, inshallah." At the time, this had the ring to me of "You should be so lucky." I had to restrain myself from saying that perhaps the way God would "will" my carpet to arrive in the U.S. would be for the merchant to actually send it!
Even more disturbing, though, is when the pre-takeoff announcements on local plane flights end with, "We will be arriving in Quetta after a one-hour flight, inshallah." Again, my thought is that I hope the pilot has some input into the result, too!
No doubt these thoughts represent personal limitations of my own. The writer Patrick O'Brian (author of a great series of seagoing novels) has a line in one of his books that goes "The sea, if it teaches nothing else, does at least compel a submission to the inevitable which resembles patience." I love that concept. Pakistan is like the sea in this regard (and to be fair to Pakistan, other developing nations exhibit the same tendency). I have at times been able to adopt behavior that "resembles patience," but I don't know what the actual sensation of patience feels like (it must truly be a virtue!). Impatience I know all too well, however. I'd like to feel patience some day, though—perhaps in my next life.
Regards, Drew
From: "Drew Remignanti, MD" <drew1r@pol.net>
Sent: June 24, 2000 7:01 PM
Subject: Pakistan Potpourri
There have been the usual ups and downs lately. On the down side, I had set up an appointment to discuss a small proposal with a hospital administrator I had met. At 10:00 a.m. I was called and told that our meeting was being rescheduled from the 10:30 we had agreed on to 1:00 p.m. When I showed up on time, his secretary said, "That meeting has been cancelled," and no further comment or explanation was offered. Having learned from experience, however, I had brought a printed-out version of my suggestion, which I was able to leave for him. A couple of days later I learned from people in our office that my contact had been arrested as part of an investigation into the fraudulent use of health-care funds (I really know how to pick the winners!). Arshad, one of the provincial surveillance officers, said the rumor is that the main culprit was this guy's boss, who had fled the country, so maybe my guy is innocent. At any rate, Arshad said he would follow up on this with my guy when he emerges or with a future administrator.
Another downer was hearing from the chief of UNICEF in Quetta about a mother with two daughters, the oldest of whom had previously had polio. But, when asked, the mother said the younger daughter had not been immunized for polio yet "because nobody has come to do it." Even worse, a local general practitioner told us he doesn't give any immunizations in his office "because a refrigerator is too expensive." Just a couple more of the obstacles here.
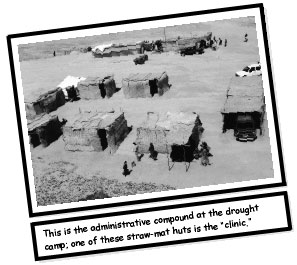
On the interesting side, I visited a "drought relief camp" (essentially a tent city) near the Afghan border. There, the government was providing food and water for a population of 10,000 nomadsrefugees, and I saw a few cases of measles for the first time.
On the up side, the people here are incredibly hospitable. They have this wonderful practice of always shaking hands hello and goodbye (or, if you're across the room and they can't easily reach you, they hold their hand over their heart). Among themselves, there is much hugging as well. It's also not unusual to see two men holding hands or draping an arm around another's shoulder while walking. I wonder if maybe they're touch-deprived, as a result of not being allowed to touch women in public. One day, one guy got a little carried away and started hugging me, too. It felt good, so I must be feeling a little touch-deprived as well!
As a function of their etiquette, though, nobody can leave a room until I do; I must always pass through doorways first. This inevitably leaves me in an unfamiliar hallway not knowing whether to go straight, left, or right (the final conversation about what we'll do next having always been in Urdu). After everyone bunches up behind me, eventually somebody comes up and gestures in the correct direction. I love a parade as much as the next person, but leading one whose route you do not know is a burden. Then, when we reach our destination, I must take the best seat in the room. Often I'm feeling hot and sweaty and just want to perch on the edge of a wooden bench and let the air circulate around me. But, no, I'm usually ushered into the upholstered seat with the wool throw-rug on it. They're quite insistent, so it's usually easiest to comply. Once a guy almost got angry with me; he was gesturing to a chair behind me and repeating, "Please sit," despite the fact that there were several people between me and the chair. I finally got seated but had to stand up to remove my pen from my pocket, since it was poking into my leg. He, of course, then had to leap up from his own seat and insist once again, "Please sit."
Another frustrating/entertaining issue is the language barrier. It is an exaggerated version of the joke about England and America being two countries separated by a common language. You can be deep into a conversation with somebody, assuming mutual understanding because you're both speaking English, only to discover at some point that you're miles apart. I've had the following exchange countless times: "Do you have cold drinks?" "Coke?" "No, Sprite please." "Sprite?" "Yes, cold, though." "Coke?" "No, Sprite, please, with ice." "Rice?" "No, ice." And so on, ad infinitum. It's a mark of my stubbornness and their courtesy that I have yet to be served Coke with rice.
I leave in less than a week, so this may be my last message. I didn't mention what follows earlier, so as to avoid creating undue worry, but I figure at this point I've probably escaped the potential dangers we were warned about in our security briefings. At the U.S. embassy briefing (we also got one from the CDC and one from UNICEF), the guy said there are seven sites in the world that are considered "critical" securitywise —and four of them are in Pakistan (Islamabad, Karachi, Peshawar, and Lahore). That, and the fact that the U.S. embassy and a United Nations building were attacked by homemade rockets fired from a converted van in the fall of 1999, got my attention (the rockets mostly hit fences and trees, though one local employee was badly injured). Also, some oil company executives were taken hostage and ultimately killed in '97. Anyway, his advice was to keep a low profile and vary our routines.
The CDC security guy had a few more bits of advice. He said using armed guards carries the risk of escalating any violence, if your guard gets trigger-happy. He also suggested that we claim to be Canadian if asked. But, knowing what a terrible liar I am, I didn't expect to deny being American unless things got really dicey.
I was even more unnerved when I talked to the U.S. guy who oversees security for Balochistan. I let him know where and when I'd be traveling, and the conversation went like this: "We don't encourage it, but for what you're doing, I guess you have to go." "Why, what's the concern?" "Bombings, tribal conflicts, drug-lords." "Bombings? When?" (I was hoping for something like '95 or '97.) "Four in April, and two or three in May so far. But they're not anti- American, just local stuff. Just keep your eyes open."
Last week there were a couple more bombings in Quetta (one of them at the bank up the street from our hotel). I was told that the bombs are set off at night, so as not to hurt people; I rarely leave the hotel at night and never alone at night. Though I've chosen to remain cautious up to the end, I have never felt personally threatened here and have concluded that staying safe in Pakistan is like doing so in New York— avoid the wrong place at the wrong time. I'll have lots more stories soon, in person.
Regards, Drew
STOP-ping communicable diseases
By Drew Remignanti, M.D., M.P.H.
STOP is the acronym for "Stop Transmission Of Polio," a program of the U.S. Centers for Disease Control and Prevention (CDC). It was initiated in 1999 to assist the World Health Organization (WHO) in its effort to eradicate polio worldwide; its director is Dr. Linda Quick. As of late 2000, there had been 220 "short-term consultants" (that's the CDC's term for STOP volunteers) who signed up to assist full-time WHO staff in one of the 30 remaining countries with endemic polio. After undergoing a one-week training period at the CDC in Atlanta, participants spend several months in their assigned country.
My road to Pakistan began in Las Vegas (a locale that may be the "anti-Pakistan") at a chance meeting with Dr. Renee Rizdon, who works in the CDC's tuberculosis-control program. She and my wife, Darby Johnson, had been classmates at Wellesley, and we were in Las Vegas for a birthday dinner for another classmate of theirs. After learning a bit from her about STOP, and having always been impressed by WHO's successful smallpox eradication campaign, I jumped at the chance to play a tiny role in wiping out polio.
The very idea of getting rid of every single copy of the literally millions of poliovirus particles spread out over the entire surface of the globe is audacious in the extreme. There are numerous examples of excellent control of infectious diseases; rabies and tetanus are just two of many. These two diseases would be bad choices for eradication, however, since the rabies virus has a large and diverse animal reservoir, while the tetanus bacterium has a spore form that can survive in soil for extended periods. There have been five separate global campaigns aimed at eradication of infectious diseases—smallpox, polio, malaria, and two less-well-known diseases called yaws and dracunculiasis.
In fact, the CDC had its beginnings in malaria-control efforts aimed at protecting U.S. soldiers during World War II. With other infectious diseases, effective vaccines have played the critical role in control or eradication, but the primary strategy in combating malaria was and is vector control—control, that is, of the insect that transmits the infectious agent (although several malaria vaccines are also currently in development).
DDT is best known today for its negative environmental impact, but its development in 1939 as a remarkably inexpensive and effective insecticide allowed for excellent control of the Anopheles mosquito, which transmits the malaria parasite. Starting in 1950, WHO assigned approximately one-third of its budget and a staff of 500 to the effort to eradicate malaria on a global basis. In India, for example, the use of DDT reduced the number of cases of malaria from 75 million to fewer than than 5 million within just a decade. And DDT use has eliminated malaria from temperate areas of the world, such as North America and Europe; well over a billion people worldwide now live in malaria-free areas that were malarious as recently as the 1950s.
However, the Anopheles mosquito's development of resistance to DDT, combined with geographic and socioeconomic limitations in developing nations, proved too great a hurdle to achieving global eradication of malaria. WHO therefore modified its goal in 1970 to control rather than eradication.
Yaws (an infection of the skin and bones caused by a spirochete bacterium) and dracunculiasis (an infection of the muscular tissue with a threadlike nematode called the guinea worm) are common in tropical and subtropical regions, though nearly unheard of in temperate areas. Again not a vaccine, but in this case the development of effective medication, is seen as the best way to eradicate yaws, while establishing clean drinking water is the only effective way of preventing dracunculiasis. The effort to eradicate yaws was also abandoned around 1970, when the discovery was made that many infected individuals do not manifest recognizable symptoms of the illness. The campaign against guinea worm infection continues at a successful pace.
The only unquestionable success to date has been the eradication of smallpox. The last U.S. case occurred in 1949, and the final case worldwide was identified in Somalia in 1977. Three years later, when intensive global surveillance had turned up no further cases, WHO declared that smallpox had been eradicated as a disease. Samples of the virus are still kept in a number of labs, including one at the CDC. But immunization against the disease has long since been suspended, and total savings in treatment and immunization costs have been estimated at $2 billion in the United States alone; since U.S. contributions to the smallpox eradication effort totaled only $32 million, this represents a significant return on investment. (By way of comparison, U.S. contributions to the malaria program were nearly $1 billion.)
It was some 200 years after Jenner's development of the smallpox vaccine before smallpox disappeared. Now, less than 50 years after Salk and Sabin developed their vaccines against polio, that disease is already near the vanishing point. The polio eradication initiative has benefited from some lessons learned in each of the preceding efforts, but it has its own hurdles to address. Unlike the case with malaria and yaws, there is no effective treatment for polio once someone is infected with the virus. And as with yaws, the phenomenon of subclinical infection—the lack of any noticeable symptoms—has to be kept in mind. In contrast to malaria, both the smallpox and polio viruses have no insect vector or animal reservoir, but there are very effective vaccines. However, the smallpox campaign was aided by the fact that smallpox vaccine was much more stable when exposed to heat than is the oral polio vaccine; in addition, smallpox immunization required only a single dose and left a visible skin mark to prove who had been vaccinated —neither of which is the case with polio vaccination.
Although progress in polio eradication is reflected in the diminishing number of polio cases reported in South Asia, the outlook for Africa is less sanguine. This is particularly true for the civil-war-ravaged countries of Angola and the Democratic Republic of the Congo. Although temporary truces have occasionally been brokered in war zones so that polio immunization efforts could continue, members of a recent STOP group in Eritrea had to be evacuated prematurely when that country's border war with Ethiopia penetrated into Eritrea.
But the effort is worth pursuing, despite the hurdles. Not only would eradicating polio have incalculable benefit in human terms, but the financial benefit would also be enormous. WHO estimates that once polio is eradicated, and immunization efforts can be suspended, $1.5 billion will be saved annually on a worldwide basis. While WHO's original goal of eradication by 2000 has been missed, the pace of current progress suggests that polio will likely be eradicated within the next several years. At a recent summit on polio at the United Nations, the target date for eradication was formally pushed back to 2002, with a goal of certification by 2005 (confidence that the virus is truly gone requires three years of intensive global surveillance, during which no new polio cases are found).
While nobody disputes the advantages of eradicating a disease, there is a counter opinion that says the substantial resources devoted to such efforts should be applied to the development of more general basic health services in developing nations, rather than to vertical, single-focus disease-eradication programs. Each approach has indisputable merits.
Anyway, I'm now back at my regular job with Granite State Emergency Physicians, staffing the emergency rooms of Elliot Hospital and Catholic Medical Center in Manchester, N.H. I expect that by the time I can again justify taking this much time away from work and home, polio will be gone, inshallah ("God willing"). But I console myself with the thought that measles eradication is the next target on the horizon.
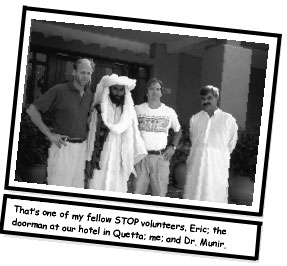
Anyone who is interested in participating in STOP, and playing a role in the final stages of the polio eradication effort, can contact Amanda White at the CDC (by phone at 404/639-8252 or by e-mail at aqw9@cdc.gov). The CDC covers travel and living costs for STOP participants, though they volunteer their time. Here we are in Islamabad—my STOP team (I'm in the white t-shirt) with Linda Quick (left), STOP's director.