
New online system for prescriptions offers safety checks
Most computer-users have come to dread error messages. But within DHMC's electronic patient record system, such messages could save lives.
More and more aspects of patients' charts are being handled electronically in the Dartmouth- Hitchcock Clinical Information System (CIS). A significant recent addition was an online prescription system and medication list. This not only circumvents the age-old bugaboo of physicians' handwriting but also provides several safety checks.
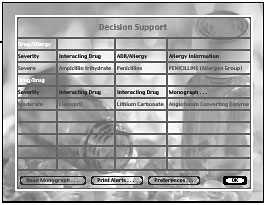
Joshua Lee, M.D., an assistant professor of medicine and a consultant to the team that created the software, says the program "allows [doctors] to see in one swoop everything else [patients are] taking and automatically checks the new prescription against medications they're already taking and against allergies they've had." If the program finds any negative interactions, it brings up a red screen with a message warning of the conflict. It's a message that could prevent a serious mistake.
|
Dosage: The program, instituted in June, also provides dosage recommendations. Errors in dosage are very easy to make, as a single decimal place can mean the difference between a therapeutic and a harmful (even lethal) quantity of medication. According to Lee, this was the most complicated element to implement, because dosage is dependent on numerous variables —from patient characteristics such as weight and renal function to the form the drug is supplied in—all of them drawn from different sources.
In addition, the system notes if a patient has recently received the same prescription. "A patient can't come and get a narcotic from one provider, then two days later show up and get it from a different provider without both knowing," explains Lee.
The system is a response to the growing complexity of medicine. There are now so many drugs on the market that it's impossible for one person to know all the interactions and dosages. Furthermore, developments in the field can occur very quickly, an ideal situation for a computer. Lee recalls a recent instance when a medication was pulled off the market by the FDA. "This occurred at about 4:00 p.m. on a Monday. By the next morning . . . we had identified everyone within the Medical Center who had received either a prescription or a drug entry for this drug, and contacted all of their primary- care providers."
The online medication software interacts within the CIS with other systems at DHMC, such as laboratory reporting and admission-data tracking. It also maintains compliance with an external standard called HL7, which is a means of making medical data understandable across different systems and platforms. "We need to be this complex because of the modern demands of patient care and the modern demands of health-care financing," explains Lee.
Unique: He says there are two "unique strengths of CIS." The first is that it "provides a tremendous amount of decision support at the time of medication documentation and prescribing in an ambulatory setting, which is new." The second is its "seamlessness of crossover between the inpatient and outpatient realms. . . . Most other systems were designed to be either one or the other," he adds, "and this clearly was done to be both."Yet despite its complexity, the system must be user-friendly for physicians. All of the information they gather while interviewing patients must be entered into the computer before the system's safety checks can be used.
"There's the hump you have to overcome to get this data in there," says Lee. "It's a new thing that people have to learn."
The CIS group has experimented with various hardware options to facilitate the entry of data. They've tried giving physicians laptops with wireless connections to the server, as well as placing fixed computers in all exam rooms. They're also testing the efficiency of using nurses to enter some data. DHMC has more than 52,000 patients with active medication lists, and over 49,000 prescriptions have been written on the system.
Clarity: There's no going back, says Lee. "I don't think we can tolerate the lack of clarity and lack of availability of data that go along with a paper chart," he says. "Nine-tenths of what you do [as a physician] is data-gathering: looking at the data and then making a decision in concert with what the patient is telling you. [To] reliably know what my patients' medical problems were, what their recent labs were, and what medications they're on, already takes me 80 percent of the way toward making clinical decisions."
Lee himself is a clinician-researcher for the digital age. He splits his time between information services, patient care, and curriculum development for residents. This means he looks at software in the context of actual practice. "We're working on these drug developments," he says, "and later that afternoon I'm seeing 10 patients in a row and writing prescriptions."
Jonathan Weisberg
If you would like to offer any feedback about this article, we would welcome getting your comments at DartMed@Dartmouth.edu.